If VT Worked, Don’t You Think We’d Do It?
BY LEONARD J. PRESS, O.D., FAAO, FCOVD JANUARY 7, 2016
There has been a steady attrition in opposition to optometric vision therapy. Perhaps it isbecause our field continually advances itself through the application of burgeoning knowledgeabout the interactions of the eyes and the rest of the brain and body. Or because our network ofcollaborators in research and clinical practice casts an ever-widening net. Possibly it’s becausepatients and parents who benefit from optometric vision therapy are increasingly pleased aboutthe outcomes. Or could it be because social media makes it difficult to suppress theaccumulated success stories that accrue every day of the week in our practices?
It is of course all of the above. Which brings me to the question posed in our title – a commentthat is on the wane but still comes up from time to time. Parents unsure about whether or not toproceed with vision therapy sometimes turn toward their pediatrician for advice. This typicallyresults in referral to a pediatric ophthalmologist for a “second opinion”. (To wit, the AAPOSsite contains the message that if vision therapy has been prescribed: “Finally, seek a secondopinion from an ophthalmologist who has the experience in the care of children recommendedby your pediatrician or primary care provider.”). The irony is that parents are often puzzledabout the second opinion they obtain, it’s usefulness akin to a consult with Dr. VinnieBoombatz.
Let’s look at what parents historically have been told when they go for a second opinion, some of which I addressed in a previously published presentation (and that we’ve debunked through a number of prior commentaries, particularly the misinformation about CI):
1. There’s no evidence that vision therapy works.
2. There’s limited evidence that vision therapy works for CI.
3. VT works for CI but it has nothing to do with learning.
4. VT works for CI but it can be done entirely at home.
5. VT works for CI but your child doesn’t have a problem.
6. Stop making excuses for your child, and get more tutoring.
7. If VT worked, don’t you think we’d do it here?
Addressing these issues through the years led me to draft responses that went into an OEPF pamphlet regarding Second Opinions About Vision Therapy. It was opinion #7 that came to
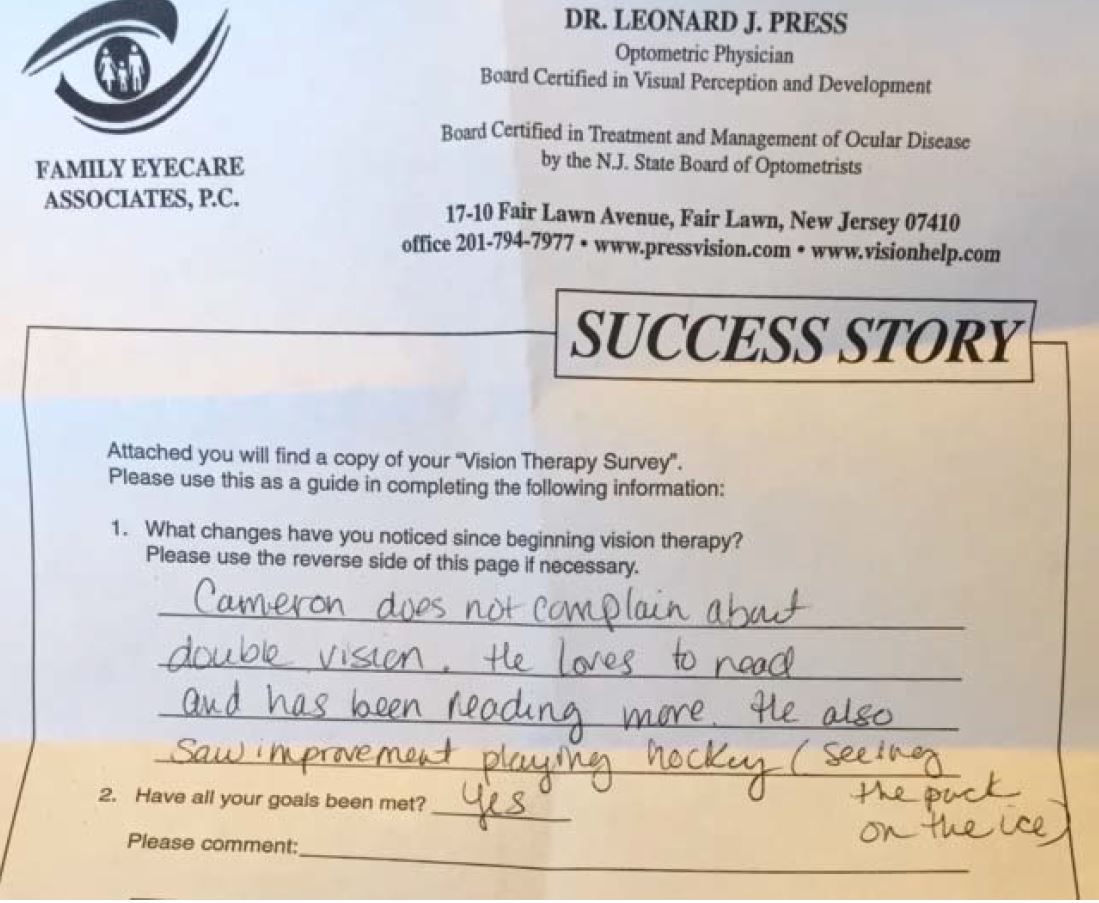
mind as I read Cameron’s Success Story above, completed by his mother. Obviously parents are increasingly able to see through biases, and to value the specialized knowledge and skill required to deliver therapy services that can:
a) eliminate double vision and severe eyestrain
b) convert avoidance of reading to willingness or passion
c) transfer to activities beyond the classroom such as sports or driving
Cameron’s experience is not unique, by any means. It’s a very similar odyssey that the American Academy of Optometry chronicled in Zach’s case, the centerpiece of this landmark position paper on Optometric Care of the Struggling Student.
So now that it has been eight years since the CITT has proven that office-based optometric vision therapy is significantly superior to home-alone therapy, Boombatzian logic should no longer reign. Why actively dissuade patients from undertaking VT with the notion that “if it worked, don’t you think we’d offer it here?”
No need to answer; the question is rhetorical. And the rhetoric implies that there is a significant price tag to offering optometric vision therapy, which includes maintaining efficient systems and well-trained staffs to render these services, and all the support functions necessary. It is increasingly incompatible with the third party insurance “here’s my co-pay” nature of busy medical practice. Rendering successful office-based optometric vision therapy is a challenge for which ophthalmologists weren’t trained, and that they wisely choose to avoid, and that is their prerogative. But don’t you think they should let patients know that?